In this section I provide a basic argument for why the term "low muscle tone" should not be part of our vocabulary and in particular should not be used as a reason why a child has movement difficulties or even worse be used as a diagnosis.
For a more detailed discussion on the topic and all the references please read: Rethinking low muscle tone
Low muscle tone as an unspecific diagnosis and label
This "diagnosis" of "low muscle tone" is usually based on the therapist's observation of a child's movement and posture.
In a survey (Martin et al 2007) of pediatric PTs and OTs in the USA the following characteristics of hypotonia were identified:
- decreased strength,
- hypermobile joints,
- increased flexibility,
- rounded shoulder posture,
- poor attention and motivation,
- leaning on supports,
- decreased activity tolerance, and
- delayed motor skill development. (Martin et al 2007)
The assumption is made that these difficulties arise, at least in part from this poorly defined concept of "low muscle tone",
Take another look at the list
These motor behaviors can all be explained by joint hypermobility and the associated muscle weakness, poor stamina and avoidance behaviors.
Importantly the underlying impairments associated with the motor behaviors in this list can be measured and addressed
- Weak muscles can be strengthened to support hypermobile joints.
- Tight muscles can be mobilized to improve posture and standing ans sitting comfort.
- Fitness training can help children overcome avoidance behavior associated having a cautious nature and avoiding effortful activity
Muscle tone as the resistance to passive movement
A muscle is said to have low tone when there is no resistance to passive lengthening, or when it feels soft on palpation.
In this instance low muscle tone refers to the inherent stiffness in the muscles and associated fascia. Importantly, it is not influenced by underlying activity in the stretch reflex.
In other words low muscle tone refers to the characteristics and structure of the muscles and related fascial structures.
What determines muscle stiffness (resistance to passive lengthening)?
Any resistance to passive lengthening of a relaxed muscle is provided by:
- Stiffness in the connective tissue structures in the muscles (about 20%)
- Elasticity of the giant muscle protein titin within the muscle cells (about 80%0 (See below)
Stiffness in the connective tissue
The many connective tissue structures within the musculoskeletal system provide the body with its basic inherent stability .
In individuals with generalised joint hypermobility the connective tissue is more compliant than usual. This increased compliance affects the:
- Joint capsule and ligaments
- Tendons
- Fascial structures – myofascia, aponeuroses, inter-muscular septa and deep fascia
In generalized joint hyerpmobility, the increased compliance in the connective tissue means that the trunk and limb segments are less stable than usual, and require more active muscle contraction to maintain stability and move joints through range.
Muscle stiffness - the role of titin
It has been estimated that up to 70 % of the passive tension in muscle comes from titin. (Fukuda et al 2008)
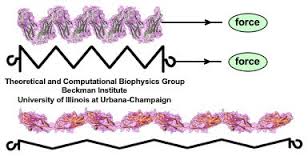 Titin is a very large elastic protein that forms part of the muscle cell. As the muscle is lengthened, the titin molecule is stretched out, producing resistance to the elongating force.
Titin is a very large elastic protein that forms part of the muscle cell. As the muscle is lengthened, the titin molecule is stretched out, producing resistance to the elongating force.
When the force is removed, the molecule recoils to its resting state. (Image ref www.ks.uiuc.edu/~ericlee/)
The titin isoform adapts to recent history by changing its size and elasticity. It increases in size following repetitive loading, with an increase in the stiffness of the muscle.
Unloading (decreased activity) decreases the size of the titin isoform, with a decrease in passive resistance to lengthening (Udaka 2008).
Quick overview of titin structure and function: Wikipedia: Titin
A muscle's resistance to passive lengthening (ie the stiffness) is therefore affected by the history of loading
Increases in loading --> increased strength + increase in passive resistance to lengthening. The muscle has more"tone".
Here is the important message
If you want to increase tone you need to work on muscle strength.
Implications for practice
A careful assessments of a child's flexibility, muscle strength, endurance, and coordination will provide clues to reasons for the postural and movement difficulties that a child experiences. Once the measurable impairments are identified and the possible environmental factors that have contributed to these impairments have been identified an effective training program that addresses impairments, function and participation can be implemented.
Bibliography and references
Martin, K., Inman, J., Kirschner, A., Deming, K., Gumbel, R., & Voelker, L. (2005). Characteristics of Hypotonia in Children: A Consensus Opinion of Pediatric Occupational and Physical Therapists. Pediatric Physical Therapy, 17(4), 275-282.
Martin, K., Kaltenmark, T., Lewallen, A., Smith, C., & Yoshida, A. (2007). Clinical characteristics of hypotonia: a survey of pediatric physical and occupational therapists. Pediatric physical therapy : the official publication of the Section on Pediatrics of the American Physical Therapy Association, 19(3), 217-26.
Fukuda, N., Granzier, H. L., Ishiwata, S., & Kurihara, S. (2008). Physiological functions of the giant elastic protein titin in mammalian striated muscle. The Journal of Physiological Sciences : JPS, 58(3), 151–9. doi:10.2170/physiolsci.RV005408
Lieber, R. L., & Ward, S. R. (2011). Skeletal muscle design to meet functional demands. Philosophical Transactions of the Royal Society of London. Series B, Biological Sciences, 366(1570), 1466–76. doi:10.1098/rstb.2010.0316

