

What can be down to improve foot posture and function?
There are two approaches to managing foot posture and function. The first is the bottom up approach: this involves the use of orthotics to support the arches of the foot in standing and in younger children may be the use of ankle boot.
The second top down approach emphasizes the importance of training flexibility of the hip and knees to allow better alignment of the foot, along with strengthening exercises and training of balance control.
In some cases an exercise program can improve the problem markedly but if the degree of joint laxity is severe foot orthotics are also needed to help maintain the foot in a fairly good posture.
|
A home based exercise program For SfA Fitness and Coordination Training Guide subscribers |
All about good foot alignment and posture
Ideally when standing the feet are be positioned parallel or wit h a few degrees of turnout with the knees facing straight forwards.
h a few degrees of turnout with the knees facing straight forwards.

The heel bone (calcaneus) is vertical and there is a small arch along the inside of the foot.


What causes flexible flat feet?
The bones of the foot are supported by very many ligaments that firmly connect the many bones of the feet.
These ligaments give the typical foot stability, hold the bones in place and support the arches.
In children with joint hypermobility (low muscle tone) the ligaments have more give than usual and do not provide the same amount of stability to the many small joints of the foot.

The ankle muscles provide further support to foot when standing.
These muscles respond rapidly to support the ankle when balance is disturbed.
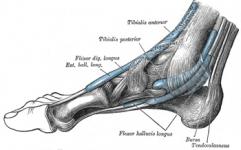
The muscles on the outside of the ankle (tibialis posterior the peronei) work to prevent the foot from tipping over to the side.
The tibialis anterior muscle stops the ankle from tilting inwards and also supports the medial arch.

The muscles that cross over the front of the ankle (tibialis anteriror and extensor digitorum longus) help to steady the foot and provide added support to the medial arch of the foot.
These muscles need to respond very quickly to any displacement of the lower leg on the foot.
In children with flat feet these muscles are often weak and slow to respond when the balance is disturbed.
Try the following
Stand upright and lean back slightly. Notice how the muscles in the front of the ankle jump into action.

Stand on one leg. Notice the small movements that occur at the ankle to maintain balance. Also notice how the knee faces more or less forwards.

Now, stand with your feet a little way apart and parallel, keeping your feet in place, move your knees closer together. Notice how this affects your medial arch - it tends to flatten.
Flat feet: angled heel bones and dropped medial arches
In children with joint hypermobility the ligaments of the foot have more give than usual which makes the foot less stable because the ligament laxity means that the foot bones are not firmly held together.
The thick band of ligamentous tissue, known as the plantar fascia, also has more give and provides less support for the medial arch when the child stands.
This tilted position of the calcaneus places further strain on, and flattening of, the medial arch.
This tilted position of the calcaneus places further strain on, and flattening of, the medial arch.
Foot alignment in standing
Children with joint hypermobility often stand with the feet turned outwards. This is caused by outwards twisting of the lower leg at the knee. This outwards twist is known as lateral tibial torsion.
When the foot is turned outwards in this way, an additional abnormal force is translated to the foot with further flattening of the medial arch.

Ankle muscle action
The tibialis anterior muscles has a particularly important role in maintaining the medial arch.
The tibialis muscles runs from the lower leg across the front of the ankle and attaches to two of the bones that form the medial arch.
When balance is disturbed the tibialis anterior muscle (along with the other ankle muscles) works to steady the leg on the foot and resist any tendency to twist the leg inwards.
The role of hip control in foot posture
At any time when all the body weight is shifted onto one leg (as happens when walking, climbing up stairs, running and so on) the muscles of the hip muscle work to control balance of the trunk over one leg and the tendency of the leg to twist inwards.
When a child with good hip muscle strength and coordination stands on one leg the trunk is upright with the pelvis horizontal and the knee facing forwards.
Small movements of the ankle help to stabilize the foot and maintain balance.
Children with joint hypermobility who have weakness and tightness of the hip muscles may have difficulty keeping the trunk erect and tend to twist the hip inwards so that the knee of the weight bearing leg faces inwards instead of forwards.
This tendency to twist the leg inwards places an additional strain on the ankle and foot making it difficult for the muscles of the ankle to work effectively to support the ankle and the foot in a good position.

Flat feet, function and pain
Not all children with flat feet experience pain with exercise. However, recent research has highlighted the link between the degree of the tilt (eversion) of the heel bone (calcaneus) and the amount of pain and dysfunction experienced by children.
The greater the degree of tilt, the more likely a child will experience foot pain.
In some cases orthotics may help to reduce pain with exercise.
What can be down to improve foot posture and function?
There are two approaches to managing foot posture and function. The first is the bottom up approach: this involves the use of orthotics to support the arches of the foot in standing and in younger children may be the use of ankle boot.
The second top down approach emphasizes the importance of training flexibility of the hip and knees to allow better alignment of the foot, along with strengthening exercises and training of balance control.
In some cases an exercise program can improve the problem markedly but if the degree of joint laxity is severe foot orthotics are also needed to help maintain the foot in a fairly good posture.
Orthotics
There are several different orthotics used to help support the foot arches and reduce pain with exercise.
Recent scientific reviews of the usefulness of orthotics in hypermobile flat feet have not found clear evidence that orthotics make a difference to pain and function in children with flat feet.
However, since some children seem to benefit from wearing orthotics it is worth a trial. In some cases all that is needed is an off the shelf arch support. In other cases a custom made support is needed. This may be include a heel cup to support the position of the calcaneus.
It is best to discuss the matter of orthotics for your child with your health professional who can make a referral to an orthotist if it is felt that it may help.
What sort of exercise training is needed?
A comprehensive exercise program for flat feet includes flexibility and strengthening exercises for the hips, knees and ankles, including:
- Stretching exercise for tight muscles and associated fascial structures
- Functional strengthening exercises for the leg and foot muscles
- Training of effective balance responses.
Physical therapy (PT) is your best option
If your child has flat feet or complains of pain in the feet when walking your best option is to consult a physical therapist for a full assessment and exercise prescription.
If the physical therapist thinks it is necessary for your child to be evaluated for orthotics she will make the necessary referral and work closely with the podiatrist/orthotist and you as parent to create a plan of action. tttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttt
|
A home based exercise program For SfA Fitness and Coordination Training Guide subscribers |
=============================================================
A very important note of caution
If your child experiences pain in the legs or feet, it is very important that first consult your health professional before embarking on an exercise program.
Disclaimer The content on this site is provided for general information purposes only and does not constitute professional advice. Read more
Selected bibliography
Evans, A. M., Rome, K., & Peet, L. (2012). The foot posture index, ankle lunge test, Beighton scale and the lower limb assessment score in healthy children: a reliability study. Journal of Foot and Ankle Research, 5(1), 1. doi:10.1186/1757-1146-5-1
Jane MacKenzie, A., Rome, K., & Evans, A. M. (2012). The efficacy of nonsurgical interventions for pediatric flexible flat foot: a critical review. Journal of Pediatric Orthopedics, 32(8), 830–4. doi:10.1097/BPO.0b013e3182648c95
Kerr, C. M., Stebbins, J., Theologis, T., & Zavatsky, a B. (2015). Static postural differences between neutral and flat feet in children with and without symptoms. Clinical Biomechanics (Bristol,
Avon), 30(3), 314–7. doi:10.1016/j.clinbiomech.2015.02.007
Kothari, a, Dixon, P. C., Stebbins, J., Zavatsky, a B., & Theologis, T. (2015). The relationship between quality of life and foot function in children with flexible flatfeet. Gait & Posture, 41(3), 786–90. doi:10.1016/j.gaitpost.2015.02.012
Kothari, A., Stebbins, J., Zavatsky, A. B., & Theologis, T. (2014). Health-related quality of life in children with flexible flatfeet: a cross-sectional study. Journal of Children’s Orthopaedics, 8(6), 489–96. doi:10.1007/s11832-014-0621-0
lunge test dorsiflex.pdf. (n.d.).
Moraleda, L., & Mubarak, S. J. (2011). Flexible flatfoot: differences in the relative alignment of each segment of the foot between symptomatic and asymptomatic patients. Journal of Pediatric Orthopedics, 31(4), 421–8. doi:10.1097/BPO.0b013e31821723ce
Rome, K., Rl, A., & Evans, A. (2010). Non-surgical interventions for paediatric pes planus ( Review ), (7).
Kothari A, Dixon PC, Stebbins J, Zavatsky AB, Theologis T. Are flexible flat feet associated with proximal joint problems in children? Gait Posture. 2016 Mar;45:204-10. doi: 10.1016/j.gaitpost.2016.02.008. Epub 2016 Feb 11. PubMed PMID: 26979907.

