Author Pam Versfeld MSc (Physio). Updated May 2024
What causes a child to walk with the feet turned inwards?
Pigeon toes, also known as in-toeing gait is usually caused by a combination of femoral anteversion and tibial torsion. Together these differences in bone growth lead to atypical torsional alignment of the leg.
Can exercises improve in-toeing?
An exercise program to improve the weakness and tightness of the hip muscles can improve not only the degree of in-toeing in standing and walking, but also improve the child's ability to perform gross motor tasks that involve walking, running, balance and jumping.
An exercise program is particularly helpful when the degree of anteversion is not severe, and may even help to accelerate the normal reduction in the angle of anteversion which occurs over time.
It must be kept in mind that an exercise program while improving strength, flexibility and function will probably not affect severe femoral anteversion to any degree. However, if a derotation osteotomy is being considered, improving a child's strength, flexibility and function before surgery will improve the outcome. (See SfA Exercise Program for Intoeing Gait)
About pigeon toes and leg alignment
A child with good leg alignment stands with the knees facing forwards and the feet parallel or turned slightly outwards. There is a slight angle between the thighs and the lower legs.

Standing with the knees and feet turned inwards
A child may stand with both the knees and the feet turned inwards.
If this is the case, then the problem may be caused by:
- tightness and weakness in the hips muscles that limit the external rotation (outwards twist) of the hip joint;
- an increase in the normal small amount of torsion (twist) in the femur - referred to as femoral anteversion. (See below.)

Standing with the knees facing forwards and the feet turned inwards
If the child stands with the knees facing forwards but the feet turned inwards, the problem lies in the rotation movements of the knees, which may also be associated with an abnormal twist in the tibia (tibial torsion).

Standing with the knees facing forwards and the feet turned out
There are also quite a number of children who stand with feet turned outwards. This outwards twist is know as lateral tibial torsion. In many children the outwards twist is related to excessive outwards rotation of the knee, along with limited inwards rotation.
Children who walk on their toes often have lateral tibial torsion associated with tightness in the iliotibial band. Read more: Idiopathic toe walking.

Standing with the knees turned in and the feet parallel
Other children stand with the knees turned in, but the feet facing forward. If this is the case, the child has a combination of medial femoral torsion and lateral tibial torsion.
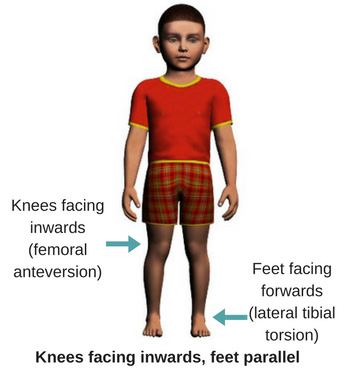 The degree of tibial torsion can best be seen when the child is instructed to stand with the knees facing directly forwards, If tibial torsion is present the feet will be positioned outwards.
The degree of tibial torsion can best be seen when the child is instructed to stand with the knees facing directly forwards, If tibial torsion is present the feet will be positioned outwards.
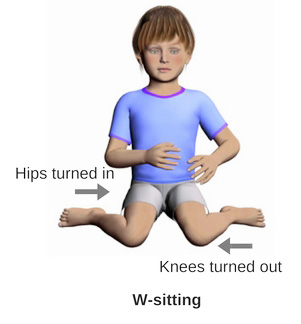
W-sitting contributes to lateral tibial torsion
Lateral tibial torsion is exaggerated in children who habitually sit between the legs (w-sitting). In this position the knee joints are forced into extreme degree of outwards rotation.
What is an in-toeing gait?
A child is said to have an in-toeing gait when he/she walks with the feet turned inwards.
The footprints of a child with good leg alignment, are angled a few degree away from the line of progression. The footprints of a child with an in-toeing gait are angled towards the line of progression.
In-toeing gait is associated with anteversion of the hips as well as hip muscle weakness and tightness.


Hip movements in children who are pigeon-toed
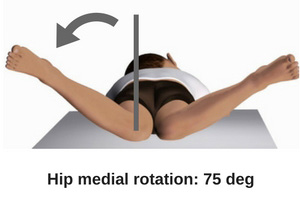
In a typically developing child, aged of 5-6 years, the rotation (twisting) movement at the hip joint allows 45 degrees in both directions. This movement is tested with the child lying on the tummy, with the hips fully extended, the thighs parallel and the knee flexed to 90 degrees.
The lower leg is moved to the left and the right. Typically, by the age of 7-8 years children have about 45 degrees of both lateral and medial rotation. (Sutherland 1988).
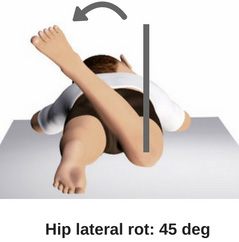

Children with in-toeing (pigeon toes) typically have increased internal (inward) rotation of the hip, often as much as 70-80 degrees, and very limited external rotation (usually only 10-20 degrees.)
What is femoral anteversion?
When a typical femur (thigh bone) is placed on a table, the lower end of the femur lies flat on the surface, and the head and neck of the femur are angled forwards slightly. This slight twist in the femur, technically known as femoral torsion, means that when standing erect with the hips in extension the knees face straight forwards.

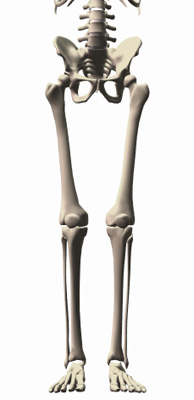
In some children the amount torsion in the femur in increased, so that the angle between a line through the head and neck of the femur and a line through the lower end of the femur increases from a typical 8-10 degrees to 30-40 degrees.

This twist in the femur means that when the head of the femur fits neatly into the hip socket (acetabulum), the knees are turned inwards.

Infant femurs are naturally anteverted
At birth the angle between the head and neck and the lower end of the femur is large (30-40 degrees). In other words infants are born with femoral anteversion. This degree of anteversion is linked to the flexed position of the infant in the womb. In fact, a full term infant's hips cannot be fully extended.
As the infant grows and develops better hip extension, and then starts to walk and becomes more active, the anteversion angle decreases, until it reaches the mature values of 8-10 degrees in adults.
This normal deroration of the femur depends on strong and balanced action of the hip muscles, in lying, standing and walking.


Link between femoral anteversion and increased hip medial rotation
In most instances, a child who has a large angle of femoral anteversion, will also have increased hip internal rotation, with decreased external rotation.
However, recent research, using MRI scans to confirm femoral anteversion, have shown that the association between the angle of anteversion and the range of hip internal rotation is variable. This means that a child with a very large range of hip internal rotation may not have excessive femoral anteversion.
Femoral anteversion can only reliably be diagnosed with an MRI or CT scan. A diagnosis cannot be made solely on the basis of increased hip internal rotation or an in-toeing gait.
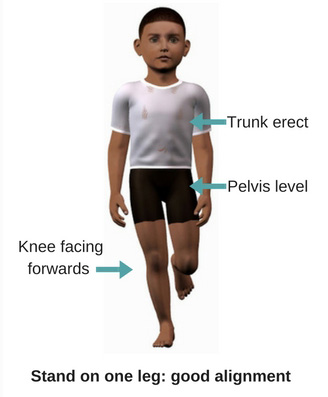
How in-toeing affects standing on one leg
By the age of 5-6 typically developing children can stand on one leg with the the trunk upright and balanced over the standing leg. The knees and feet face forwards, and the child uses small movements of the foot to maintain balance.
Children with limited range of hip external rotation, along with some tightness in the iliotibial band and weakness of the buttock muscles have difficulty standing on one leg with good alignment.
The pelvis and trunk tilt sideways and the knees tend to turn inwards. The child uses hip and trunk movements to maintain balance, rather than the more effective small ankle movements.

In-toeing and the swing phase of gait
Children who walk with the feet twisted inwards usually have difficulties with controlling the position of the foot as the leg is moved forwards to take the next step. The thigh and the foot are turned inwards as the leg is moved forwards and placed down on the floor.
This inwards twist of the leg is associated with weakness of the hip muscles that flex and rotate the hip joint.

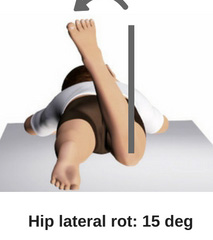
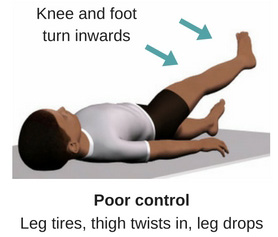
Try the following
The difficulties a child experiences with controlling the rotation of the hip in walking, can be seen when a child is asked to lie on the back, lift one leg to 450 and hold the position for 20 seconds. If the child has good strength in the hip flexor muscles the knee will face upwards and the position can be easily maintained for the full 20 seconds.
If the hip flexor muscles are weak child tends to twist the leg inwards so that the knee faces inwards as the muscles get tired.

Does in-toeing improve over time?
Orthopedic surgeons tend to recommend a wait-and-see approach for young children presenting with in-toeing gait The expectation is that the degree of in-toeing will decrease over time and have corrected itself by the age of 8-10 years.
And indeed research has shown that the degree of in-toeing when walking does often improve over time. However the tendency for the thighs to be twisted inwards with the knees turned towards each other when standing and walking may still be present, even when the feet are not turned inwards when standing and walking.
This is because the child compensates for the inwards twist of the thigh by twisting the lower leg outwards at the knee joint.
When intoeing is associated with femoral anteversion
If the in-toeing is severe and interferes with function, and there is marked anteversion of the femur, the child's orthopedic surgeon may recommend a derotation osteotomy to correct the twist in the femur.
An MRI or CT scan is needed to establish a diagnosis of anteversion of the femur. It is important to note that while in most cases and increased anteversion angle is usually associated with excessive internal rotation of the hip, this may not always be the case. (Kim et al 2011)
The opposite is also true, a large angle of hip internal rotation does not necessarily mean that femoral anteversion is present.
In severe cases of femoral anteversion, most often seen in children with cerebral palsy a derotation osteotomy improves the biomechanics of the hip joint and allows the muscles to start working more effectively when walking.
Can exercises improve in-toeing?
An exercise program to improve the weakness and tightness of the hip muscles can improve not only the degree of in-toeing in standing and walking, but also improve the child's ability to perform gross motor tasks that involve walking, running, balance and jumping.
An exercise program is particularly helpful when the degree of anteversion is not severe, and may even help to accelerate the normal reduction in the angle of anteversion which occurs over time.
It must be kept in mind that an exercise program while improving strength, flexibility and function will probably not affect severe femoral anteversion to any degree. However, if a deroration osteotomy is being considered, improving a child's strength, flexibility and function before surgery will improve the outcome.
A program of exercises to improve pigeon toes (in-toeing) when standing and walking
The SfA exercise program includes exercises designed to improve the impaired flexibility, muscle strength and coordination commonly experienced by children who stand and walk with in-toeing.
Children will only participate in an exercise program if it is interesting, there is a bit of a challenge and they experience success. All exercises start with an easy version and provide instructions for increasing the difficulty.
Hip muscle stretching exercises to improve the ability to extend and laterally rotate the hip joint
Standing on one leg exercises: to improve the ability to stand on one with good pelvic and leg alignment.
Hip flexion exercises: to improve the child's ability to lift the leg forwards with the foot straight.
Walking exercises: to improve foot placement, balance and coordination.
Subscribers can access the program of exercises here:
Training program for children with in-toeing
Subscribe to the SfA Fitness and Coordination On-line Training Guide
Includes PDF files for home exercise programs (HEPs).
Disclaimer: The content on this site is provided for general information purposes only and does not constitute professional advice.
Bibliography
Botser IB, Ozoude GC, Martin DE, Siddiqi AJ, Kuppuswami S, Domb BG. Femoral anteversion in the hip: comparison of measurement by computed tomography, magnetic resonance imaging, and physical examination. Arthroscopy. 2012 May;28(5):619-27. doi: 10.1016/j.arthro.2011.10.021. Epub 2012 Feb 1. PubMed PMID: 22301362.
Sielatycki JA, Hennrikus WL, Swenson RD, Fanelli MG, Reigha J, Hamp JA. In-Toeing Is Often a Primary Care Orthopedic Condition. J Pediatr. 2016 Jul 25. pii: S0022-3476(16)30382-1. doi: 10.1016/j.jpeds.2016.06.022. [Epub ahead of print] PubMed PMID: 27470689.
MacWilliams BA, McMulkin ML, Davis RB, Westberry DE, Baird GO, Stevens PM. Biomechanical changes associated with femoral derotational osteotomy. Gait Posture. 2016 Jul 1;49:202-206. d
Sutehrland DH et al (1988) The Development of Mature Walking. Mac Keith Press
Mooney JF 3rd. Lower extremity rotational and angular issues in children. Pediatr Clin North Am. 2014 Dec;61(6):1175-83.
Kim HD, Lee DS, Eom MJ, Hwang JS, Han NM, Jo GY. Relationship between Physical Examinations and Two-Dimensional Computed Tomographic Findings in Children with Intoeing Gait. Ann Rehabil Med. 2011 Aug;35(4):491-8.
Radler C, Kranzl A, Manner HM, Höglinger M, Ganger R, Grill F. Torsional profile versus gait analysis: consistency between the anatomic torsion and the resulting gait pattern in patients with rotational malalignment of the lower extremity. Gait Posture. 2010 Jul;32(3):405-10. doi:
Howlett JP, Mosca VS, Bjornson K. The association between idiopathic clubfoot and increased internal hip rotation. Clin Orthop Relat Res. 2009 May;467(5):1231-7.

